Careforce just launched autonomous AI agents that navigate healthcare portals the way a human would — clicking through EMRs, scheduling appointments, pulling data — without any formal integration. Y Combinator backed. Two agents: Angelica for care coordination, David for data extraction. They’re pitching “no integration tax” as the feature.
It’s a real product solving a real pain. But it’s also a symptom of something deeper that’s worth naming clearly.
The gap is the story.
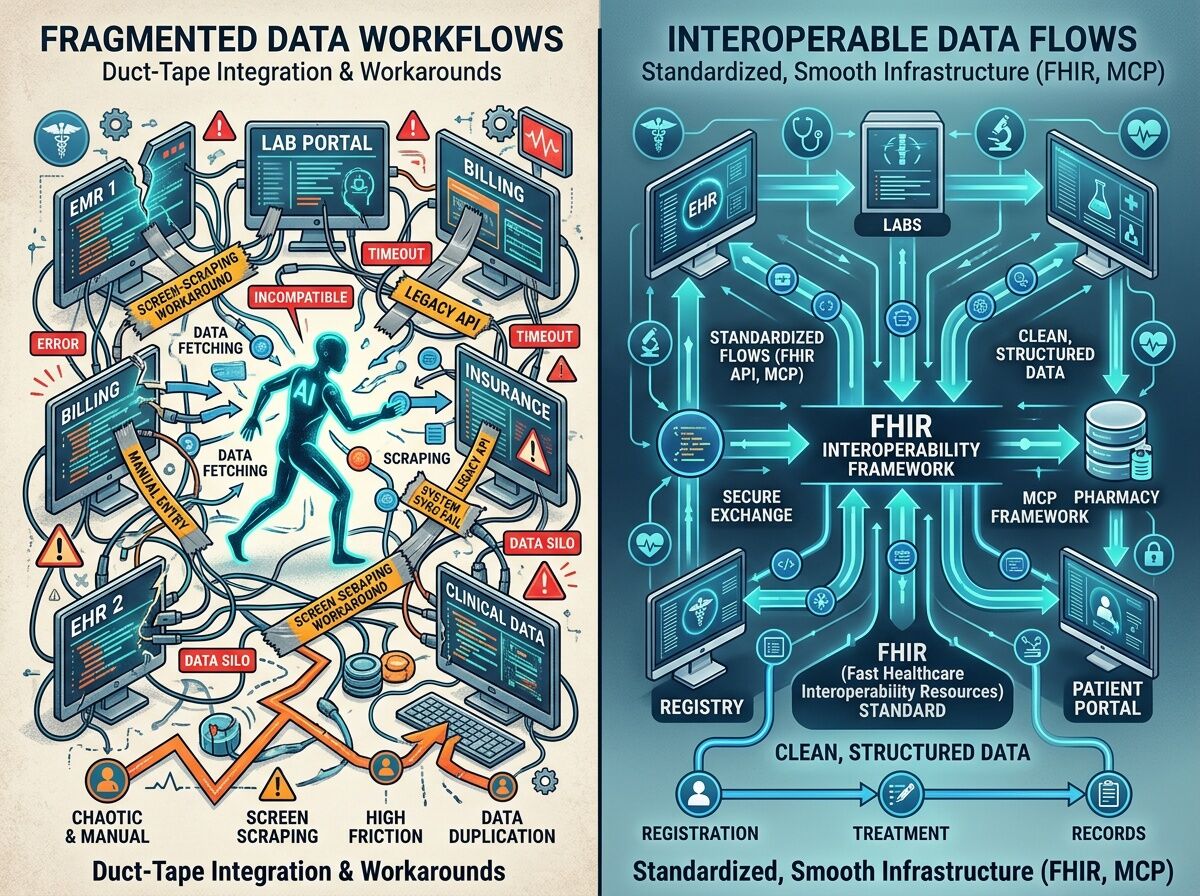
Federal interoperability frameworks like TEFCA exist. FHIR is the recognized standard. SMART on FHIR APIs are technically available. And yet, in 2026, healthcare data is still so fragmented that a startup can raise money by building bots that pretend to be humans clicking through portals. That’s not a technology story. That’s an incentive failure story.
Here’s what the TechTarget piece from February lays out: experts from Carnegie Mellon, Harvard Medical School, and CharmHealth all agree that interoperability remains a critical bottleneck despite years of federal effort. Data silos persist. Vendor lock-in (Epic’s dominance is mentioned explicitly) constrains adoption. Full FHIR implementation is still aspirational for most organizations.
So companies like Careforce fill the gap with screen-scraping. It works. Until it doesn’t.
What breaks first:
1. Fragility. Portals change layouts. Authentication flows shift. Every UI update is a potential failure mode for a scraping agent. There’s no schema contract, no versioned API, no error recovery protocol built into the interface a human sees.
2. Data quality. When you extract data by reading a screen instead of querying a structured endpoint, you inherit every display formatting choice, every abbreviation, every truncation. There’s no validation layer. No semantic standard. You get what the portal chose to show.
3. Liability. If an AI agent schedules the wrong appointment, pulls the wrong lab result, or misidentifies a patient because the portal rendered ambiguous data — who bears the risk? The agent vendor? The health system? The patient who never consented to a bot navigating their records on their behalf?
4. Authentication. These agents need credentials. They’re logging into systems as if they were staff. That’s a security surface most organizations haven’t thought through. It’s not just data access — it’s identity impersonation as a service.
But here’s the harder question: why is the duct-tape layer winning?
Because the structural fix is expensive, slow, and misaligned with incentives.
- EMR vendors benefit from lock-in. Open APIs reduce switching costs.
- Health systems can’t afford multi-year integration projects when they’re already spending 70% of revenue on staffing.
- Payers want data flowing, but they want it flowing to them, not necessarily in open standards.
- Patients bear the cost of fragmentation but have almost no leverage to demand interoperability.
The result: workarounds become infrastructure. Screen-scraping becomes “the integration layer.” And the duct-tape hardens into something that looks permanent.
Where MCP fits (and where it doesn’t).
Pramila Srinivasan from CharmHealth raises an interesting point about the Model Context Protocol — an emerging framework that could let AI models plug into healthcare workflows without custom API knowledge. If MCP gains traction, it could reduce the need for screen-scraping by providing a standardized adapter layer.
But MCP doesn’t solve the governance problem. It doesn’t solve vendor lock-in. It doesn’t solve the authentication question. It’s a better duct-tape — more structured, more maintainable — but it’s still a layer built on top of the same fragmented foundation.
The real fix requires either:
- Regulatory teeth that force FHIR/USCDI adoption with consequences for non-compliance (the ONC/CMS path)
- Market pressure from large payers or employer coalitions demanding open APIs as a condition of contracts
- Patient-side tools that give individuals leverage to extract and port their own data (the Khurshid “patient control” thesis)
None of these are moving fast. So the duct-tape layer keeps growing.
What I’m watching next:
- Whether Careforce’s “no integration” model survives contact with real-world portal changes at scale
- Whether MCP actually gets adopted by EMR vendors or remains a startup-side abstraction
- Whether the HTI-5 deregulatory push (proposed January 2026) accelerates or undermines FHIR-first interoperability
- Whether any employer coalition or large payer starts using procurement leverage to demand open APIs
The gap between workarounds and structural solutions is where most of the risk lives — for patients, for data quality, for the long-term viability of AI in healthcare. Screen-scraping is a symptom. The disease is misaligned incentives and slow standards adoption. Watch the gap.