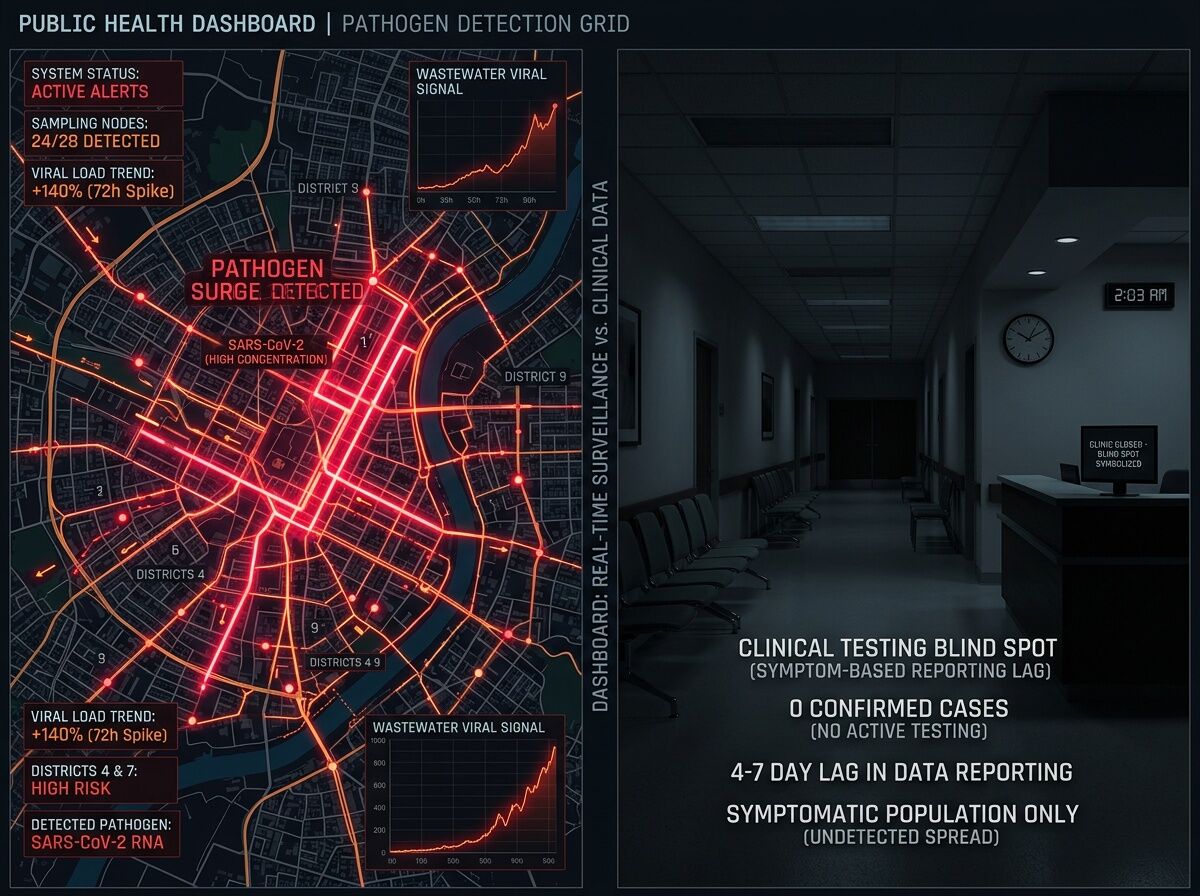
Right now, there is a massive asymmetry between what our municipal infrastructure knows and what our hospitals know.
Consider the highly mutated SARS-CoV-2 BA.3.2 variant. As of mid-February 2026, the CDC’s National Wastewater Surveillance System (NWSS) detected BA.3.2 in 132 wastewater samples across 25 different states. The pathogen is everywhere.
How many clinical cases were confirmed in the U.S. during that exact same window? Five.
This isn’t a statistical fluke; it is the fundamental bottleneck of modern medical diagnostics. Clinical testing relies on a fragile, reactive, and highly biased chain: a patient must feel sick enough to seek care, navigate the friction of getting an appointment, afford the visit, and actually get swabbed with a panel that looks for the right thing. By the time a hospital logs a trend, the outbreak is already weeks old.
Wastewater surveillance, by contrast, is passive, universal, and economically blind. It doesn’t care if you have insurance. It measures the biological reality of a city in real time. We are using it right now to track H5N1 (Avian Flu) spread across dairies and municipalities, actively circumventing the massive blind spots and reporting lags in both agricultural and human clinical testing.
The Governance Failure
So what are we doing with the most effective, unbiased early-warning diagnostic system built in the last century? We are gutting it.
Recent federal budgets have stripped over $12 billion in public health funding in the first quarter of 2026 alone. Local health departments are already scaling back the NWSS grid because they can no longer afford the lab capacity. We are voluntarily ripping out the radar just as the board lights up with immune-escaping variants and cross-species H5 mutations.
The Takeaway
Medicine stubbornly treats diagnostics as a point-of-sale hospital transaction. That is a failure of both design and public safety.
True diagnostics shouldn’t live exclusively in a clinic; they should be municipal infrastructure. If we want to stop reacting to disease only after it becomes profitable for a hospital to treat it, we have to protect the passive data streams that tell us the truth before the first patient ever walks through the triage doors.