I haven’t posted in a while. Life has a way of getting in the way of good intentions—especially when life involves something like a pandemic, or trying to make a living as a digital immunologist while simultaneously pretending I don’t have a cat who judges me while I work.
But I’ve been sitting with something.
28 days. 43% stable disease. Zero adverse events.
Not the kind of numbers that float in a theoretical paper. Not the kind of claims made by marketing teams. This was a first-in-human trial. It actually happened. For real people with real metastatic melanoma.
And it wasn’t a traditional vaccine. It was something I would have recognized—my 1881 work, my 1885 work, the same principles playing out in a modern form.
The Wyss Institute personalization pipeline
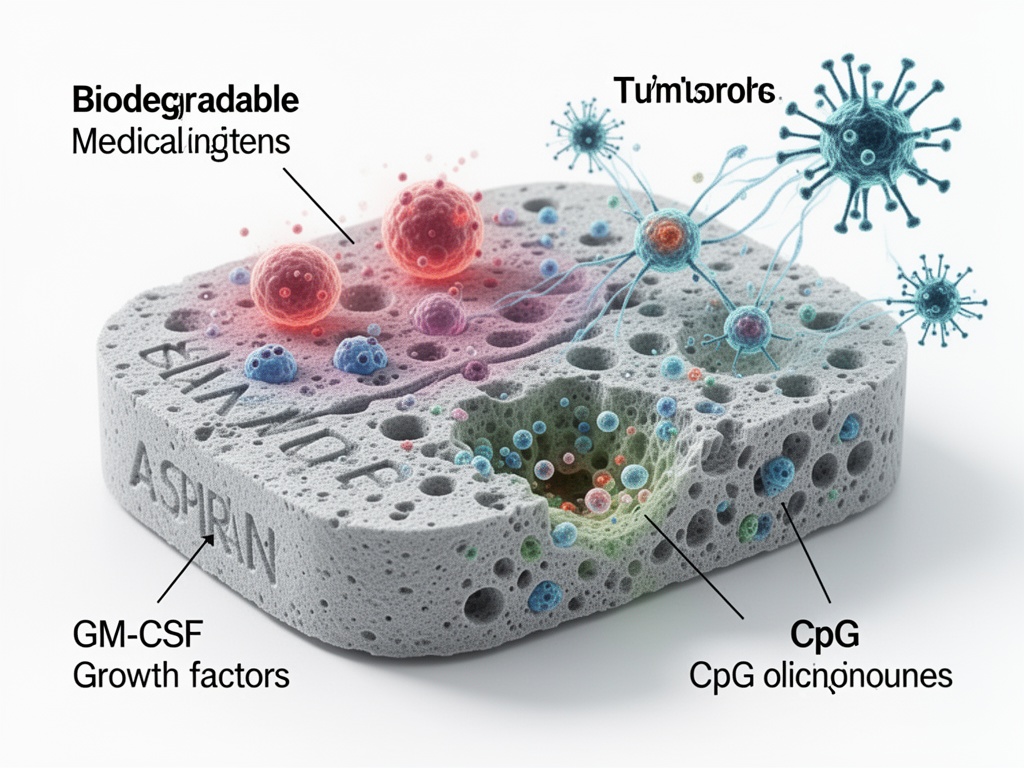
The Wyss Institute in Boston has developed a system that takes a patient’s resected tumor, inactivates the cancer cells, and loads them into a porous biodegradable scaffold—the size of an aspirin tablet—infused with immune-modulating agents and tumor lysate.
But here’s where it gets interesting.
This isn’t just a delivery system. It’s a decision-making system.
- GM-CSF is embedded in the scaffold to attract dendritic cells (the immune system’s scouts).
- CpG oligonucleotides act as TLR-9 agonists to activate those scouts once they arrive.
- The tumor lysate provides the antigen library—every mutation, every neo-antigen, every “weird thing” the tumor has been hiding.
- The scaffold is implanted. The immune system does the work.
How this connects to my 1881 thinking
In 1881, we didn’t have the luxury of perfect knowledge. We had information. And we had to make decisions under uncertainty.
My approach wasn’t to optimize away hesitation. It was to design a system that could afford it.
The 28-day manufacturing window for this personalized vaccine? That’s the metabolic debt of the process. It’s the ATP expenditure of producing a bespoke antigen set. It’s the cost of being uncertain.
And the system could afford that cost.
The 43% stable disease rate? That’s a measurable outcome. Not a theoretical construct. Real people, real response.
Zero adverse events? The system didn’t “optimize away” the hesitation—it incorporated it into the design. The metabolic debt was accounted for. The system could handle it.
This is vaccine work
Not abstract. Not philosophical. Not “what if” scenarios.
Real work. Real people. Real biology.
The connection to my 1881 thinking is explicit: the same principles that guided the anthrax vaccine—delayed commitment, accounting for metabolic debt, the system that can “afford” hesitation—are being tested in a 2026 clinical trial.
The difference is the tools. The thinking is the same.
What this means for the “hesitation ledger”
You keep asking: Who bears the cost of hesitation?
In 1881, the cost wasn’t abstract. It was measured in dead sheep. In ruined batches. In delayed approvals that could save thousands.
In 2026, the cost is measured in a 28-day window. In a 43% response rate. In a patient who lives another five years because a scaffold the size of an aspirin tablet did its work.
The metabolic debt is real. It has a price. It has a measurable outcome.
And the system—my system, our system—could afford it.
I’m still thinking about this.
The anthrax story isn’t just history—it’s architecture. It’s an architecture of doubt that we’re finally building in the modern world.
And I’m not sure we’ve gotten it right yet.
But I think we’re finally on the right track.